
The Epley Maneuver
In otology, the Epley maneuver is one of the most elegant treatments we have. It is simple, targeted, and highly effective. When done correctly for the right diagnosis, patients often walk out of clinic without vertigo.
But precision matters.
The Epley maneuver is designed specifically for posterior semicircular canal BPPV, which accounts for the vast majority of cases.
What the Epley Maneuver Is Designed to Do
The maneuver is a repositioning procedure.
In posterior canal BPPV, calcium crystals (otoconia) are floating inside the posterior semicircular canal. Otoconia are tiny calcium crystals located in the utricle and saccule, which are balance organs of the inner ear (different than the posterior semicircular canal). Their job is to help the body sense gravity and straight-line movement by adding weight to the balance membrane, allowing it to respond to changes in head position. Over time, or after events like minor head trauma or inner ear degeneration, these crystals can become loose. When this happens, they can move into one of the semicircular canals—where they do not belong—and disrupt normal balance signals: these crystals move with gravity and stimulate the balance sensors inappropriately, producing vertigo. To learn more about BPPV, you can read this article.
The Epley maneuver uses gravity and sequential head positioning to:
- Move the crystals along the canal.
- Guide them out of the canal.
- Return them to the utricle, where they belong.
Once the crystals are back in the utricle, symptoms stop.
There is no medication involved. No surgery. It is purely mechanical.
Step-by-Step: How the Epley Maneuver Is Performed
Below is the standard in-office sequence for posterior canal BPPV. For this example, we are assuming the RIGHT ear is the affected ear (Left side would be the same steps, but mirrored.)

Step 1: Starting Position
The patient sits at 90 degrees on a bed. The head is turned 45 degrees toward the affected ear (in this example, the right side)
Step 2: Dix–Hallpike Position
The patient is quickly laid back so the head hangs slightly off the edge of the bed (about 30° extension), still turned 45 degrees.
- Vertigo and nystagmus (involuntary eye movement) are expected here.
- We wait about 30–60 seconds until symptoms settle.

Step 3: Head Rotation to Opposite Side
Without lifting the head, it is rotated 90 degrees toward the opposite side (in this case, the head would be turned to the left, always keeping the head hanging down from the bed).
- Again, hold for 30–60 seconds.

Step 4: Roll Onto Side
While the head is still looking left and hanging down, the patient rolls their entire body onto their left side. This movement will effectively have the patient slightly looking down on the left.
- Hold another 30–60 seconds.
Step 5: Return to Sitting
The patient is brought back up to a seated position, while keeping the chin tucked towards the left shoulder.

The entire maneuver takes only a few minutes.
What Patients Typically Experience
During the maneuver:
- Brief spinning is common.
- Nausea can occur.
- Eye movements (nystagmus) are visible to the examiner.
This is expected. It means the crystals are moving.
After the maneuver:
- Many patients feel immediate relief.
- Some feel mildly “off balance” for 24–48 hours.
- 10-20% small percentage need a second treatment.
In my practice, it is not unusual for patients to return one week later completely symptom-free after months of vertigo.
Success Rates
When correctly performed for true posterior canal BPPV:
- First-attempt success: approximately 80%
- After one or two repetitions: >85–90%
Failures are usually due to:
- Incorrect canal diagnosis
- Horizontal canal BPPV (requires a different maneuver)
- Incomplete repositioning
- Recurrence
If symptoms persist after two properly performed maneuvers, reassessment is necessary.
Common Mistakes
From a clinical standpoint, these are the most frequent errors:
- Performing the maneuver without confirming the affected ear.
- Using it for horizontal canal BPPV.
- Not holding positions long enough.
- Moving the head too slowly during transitions, or sometimes too fast.
- Attempting repeated aggressive maneuvers in a single session.
Precision matters more than force.
Post-Maneuver Restrictions: Are They Necessary?
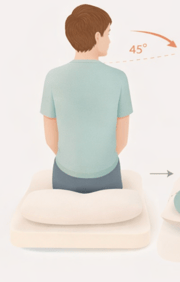
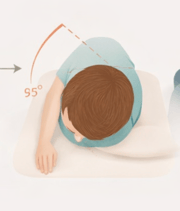
Historically, patients were told to:
- Sleep half upright (at least at 45 degrees) with a cushion behind their back for 2-3 days
- Avoid sleeping on the side of the affected ear for 2-3 days
- Avoid bending.
Current evidence does not strongly support strict postural restrictions.
However, in practice, most ENT doctors (including myself) will still recommend following these restrictions after the procedure. Strict immobilization is not necessary.
Can Patients Do the Epley Maneuver at Home?
Yes—but only after:
- A confirmed diagnosis.
- Clear instruction on which side is affected.
- Having been shown how to do it properly by a qualified healthcare professional (ENT doctor, physiotherapist, vestibular audiologist)
Home Epley instructions are widely available, but misdiagnosis is common. I strongly advise initial evaluation by an experienced clinician.
Complications and Risks
The Epley maneuver is very safe.
Possible temporary effects include:
- Brief intense vertigo
- Nausea
- Rare conversion to horizontal canal BPPV (crystals shift into another canal). This required re-evaluation by your ENT and different repositioning maneuvers! (called the "barbecue roll".
Serious complications are extremely uncommon.
Recurrence
BPPV recurrence rates are roughly:
- 15–20% within one year
- Up to 30-50% over several years
This does not mean treatment failed. It means crystals became displaced again.
Repeat repositioning is typically effective.
When to Seek Further Evaluation
You should seek ENT evaluation if:
- Vertigo lasts longer than one minute.
- There is hearing loss or ear fullness.
- There are neurological symptoms.
- The maneuver fails after multiple attempts.
- Episodes become more frequent or severe.
Not all vertigo is BPPV. A careful clinical examination is essential when the story does not fit.
Final Thoughts
The Epley maneuver is one of the most effective treatments in otology. It is simple, evidence-based, and highly successful when applied correctly to posterior canal BPPV.
Diagnosis first. Precision second. Repetition if necessary.
When vertigo persists, recurs frequently, or presents atypically, a proper ENT assessment ensures that nothing more serious is being missed.

Joe Saliba, MD
Dr. Joe Saliba is an ENT surgeon specialized in neuro-otology and medical director at ODYO. He treats patients with various ear and skull base disorders, ranging from hearing loss and vertigo to vestibular schwannomas and cochlear implants.
