
What Is a Meningocele? What Is a Meningoencephalocele?
The brain is housed inside the skull and wrapped in protective coverings called the meninges.
These coverings are made of three layers. The outermost and thickest layer is called the dura. The meninges — and especially the dura — act like a secure barrier. They keep the cerebrospinal fluid (CSF) contained within the brain’s compartment.
CSF is a clear thin fluid (it looks like water, but has a salty taste) that surrounds the brain. It cushions the brain, helps absorb shocks, and provides an important layer of protection.
A meningocele is a herniation (outpouching) of only the meninges through a defect in the skull base.
A meningoencephalocele is more significant — both meninges and a small portion of brain tissue herniate through the defect.
Because the bone that houses the ear (called the temporal bone) sits directly beneath the brain cavity, any herniation (bulging) of the brain’s protective lining — or, in more severe cases, of brain tissue itself — can push downward into nearby ear spaces. Specifically, this herniated tissue can extend into:
-
The mastoid cavity: the air-filled portion of the temporal bone located just behind the ear
-
The middle ear space: the small, air-filled chamber behind the eardrum that contains the hearing bones (ossicles)
If the protective barrier is breached enough for CSF to escape, the patient develops a CSF leak (also called CSF fistula).
The moment CSF communicates with the middle ear or ear canal, bacteria have a pathway toward the brain. That is the clinical concern.
Understanding the Anatomy
To understand this condition, you must visualize the anatomy clearly. This image will help you do so:
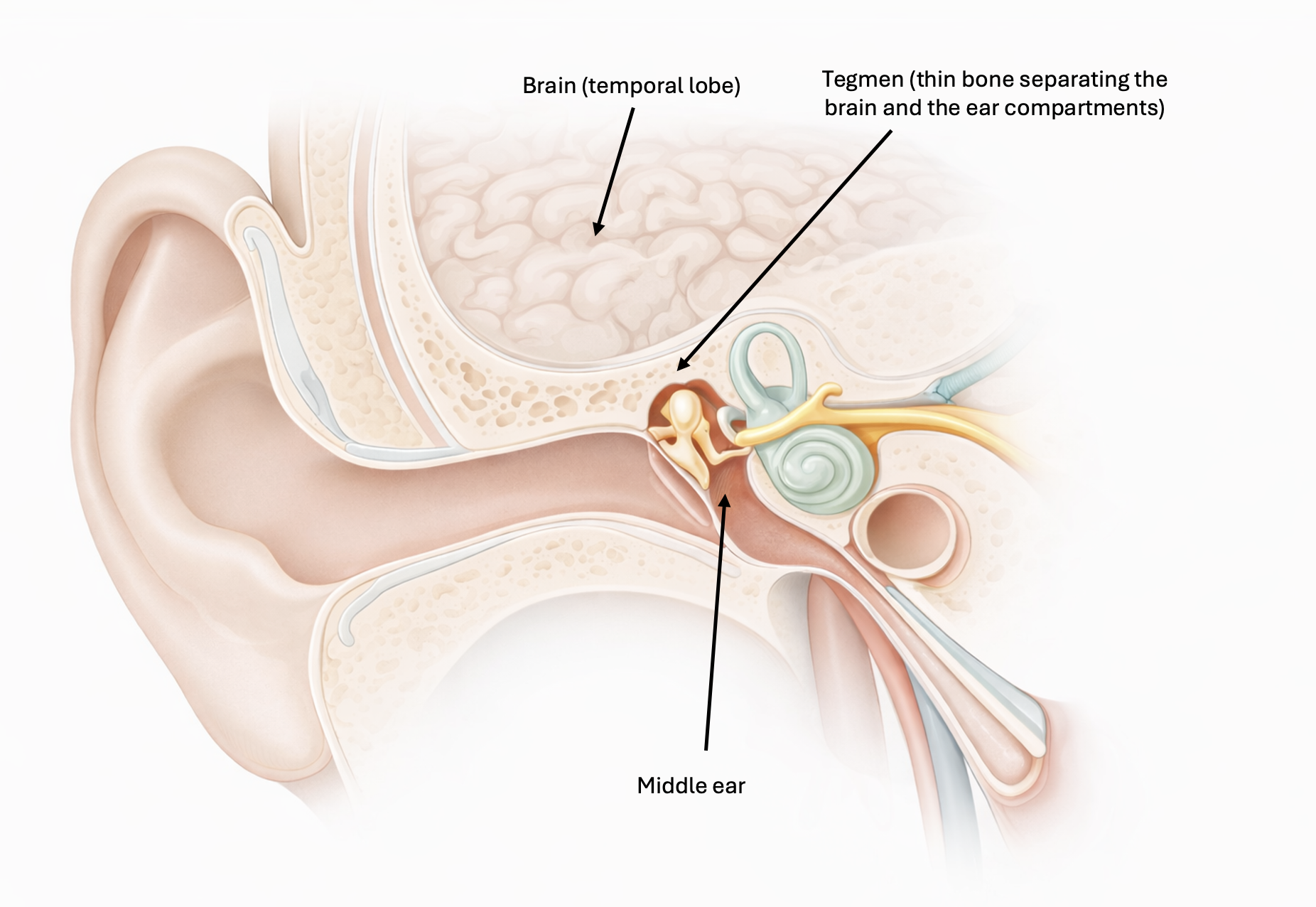
The roof of the middle ear and mastoid is called the "tegmen". It is a thin plate of bone separating the brain from the ear.
Above it:
- Brain
- Meninges
- CSF
Below it:
- Middle ear
- Ossicles (hearing bones)
- Mastoid air cells
If the tegmen develops a defect, called a dehiscence (hole or thinning), meninges — and sometimes brain tissue — can herniate downward.
How Do Ear Meningoceles Form?
There are three main mechanisms.
Spontaneous (Most Common)
This is the most common scenario in adults.
Typically:
- Middle-aged
- Overweight
- Often women
- May have features of idiopathic intracranial hypertension (elevated brain pressure without a tumor)
Over time, the chronic pulsations of the brain (and elevated pressure) erodes the thin tegmen bone. Eventually, a defect forms.
This is a slow mechanical process — not an infection and not a tumor.
Acquired Causes (that develop due to a condition)
These are more common in adults:
- Chronic ear infections, leading to thinning of the tegmen bone over time
- Prior ear surgery
- Trauma that involves the base of the skull
- Skull base tumors
- Chronic increased intracranial pressure
Congenital (Present from Birth)
Some patients are born with thinning or small defects in the skull base. This is an uncommon scenario in adults.
How Does a CSF Leak Occur?
CSF is under constant low pressure in the brain compartment. When a bony defect forms and the meninges herniate through it, the protective barrier of the brain that keeps the CSF barrier (the dura) weakens.
If the dura tears, CSF escapes the brain compartment and can spread elsewhere:
- Can enter the middle ear
- Can drain through the eustachian tube into the nose
- Can leak through a perforated eardrum or through an ear tube
Patients may report:
- Persistent clear ear drainage (thin, like water)
- A feeling of fluid in the ear
- Salty or metallic taste in the throat
- Clear watery dripping from the nose when the head is bent over
- Hearing loss and ear fullness
Clear drainage that tests positive for beta-2 transferrin confirms CSF. Beta-2 transferrin is a protein found almost exclusively in CSF. It is highly specific.
Clinical Presentation
Patients may present in different ways.
Meningocele and Meningoencephalocele
The most common presentation of meningoceles and meningoencephaloceles is ear fullness, hearing loss and pulsatile tinnitus. Headache can be reported (if intracranial pressure is elevated).
In some patients, there are no symptoms at all, until they get an otitis (ear infection) that becomes a meningitis. Then, a work up is done and reveals the underlying issue.
Meningocele/ Meningoencephalocele with CSF leak
Once a CSF leak occurs, patients will usually report:
- A feeling of fluid in the ear
- If a tube is placed in the ear: persistent clear ear drainage (thin, like water)
- Salty or metallic taste in the throat (leaking through the Eustachian tube into the throat)
- Clear watery dripping from the nose when the head is bent over
- Hearing loss and ear fullness
- History of repeated meningitis in the past
Diagnostic Workup
This is not a clinical diagnosis alone. Imaging is essential.
High-Resolution CT Scan of the Temporal Bone
CT defines the bone anatomy.
This shows:
- The exact location and size of the bony defect in the tegmen
- Fluid build-up in the mastoid bone
- The relationship between the brain tissue that is herniated and the hearing bones and the inner ear
- The overall anatomy of the ear
MRI of the Temporal Bone
MRI defines the nervous system (brain) tissue:
- Confirms whether there is herniated brain tissue, or only meninges (or neither)
- Signs of CSF extending into mastoid and middle ear
Beta-2 Transferrin Testing
Fluid from the ear is collected and analyzed.
Positive result = diagnostic for CSF.
Audiogram
Typically shows:
- Conductive hearing loss (due to fluid buildup and from the brain tissue impeding movement of the ossicles in the middle ear)
- Sometimes mixed loss
To learn more about audiograms, read this article.
Evaluation for Intracranial Hypertension
If suspected:
- Ophthalmology exam (to rule out optic nerve swelling)
- Possibly lumbar puncture (carefully selected cases). I refer these patients to neurology for further evaluation.
Treatment: Surgical Repair
Why This Condition Matters
The primary risk is meningitis.
Bacteria from the ear or nose can travel upward into the intracranial space.
Patients with untreated CSF leaks have:
- Recurrent meningitis risk
- Progressive enlargement of defect
This is not a condition to observe long-term. Once confirmed, treatment is surgical and is strongly recommended.
There is no effective medical therapy to permanently stop a CSF leak from a skull base defect.
Surgical Goals
- Remove herniated brain tissue (usually nonfunctional and scarred down)
- Repair the skull base bony defect
- Repair the CSF leak by re-creating a watertight seal of the defect in the meninges
- Improve hearing
Surgical Approaches
Depending on defect size and location:
- Transmastoid approach (through the mastoid bone, the bone of the ear)
- Middle cranial fossa approach (from above, by opening the skull over the ear)
- Combined approach (for large defects)
To repair the bony defect, we use a step-by-step, multilayered reconstruction. This means rebuilding the area in several thin layers using a combination of:
-
Autologous (which comes from the patient himself) bone graft
-
Cartilage (also from the patient)
-
Fascia (connective tissue) from the patient
-
Synthetic dural substitutes
In patients with elevated intracranial pressure, management of pressure is also important.
When performed correctly, success rates are very high.
When Should Patients Seek Evaluation?
Immediate evaluation is warranted if:
- Clear persistent ear drainage
- Recurrent meningitis
- Unexplained middle ear fluid without infection
- Clear drainage after ear surgery or trauma
This is not something to ignore.
Final Thoughts
Ear meningoceles and CSF leaks are uncommon but important conditions in otology. They represent a failure of the skull base structures, between the brain and the ear. The diagnosis requires careful imaging and laboratory confirmation. The treatment is surgical — and when properly performed, it is highly effective.
If there is persistent clear ear drainage or unexplained middle ear fluid, an ENT evaluation is essential. Early recognition prevents meningitis and restores long-term safety.

Joe Saliba, MD
Dr. Joe Saliba is an ENT surgeon specialized in neuro-otology and medical director at ODYO. He treats patients with various ear and skull base disorders, ranging from hearing loss and vertigo to vestibular schwannomas and cochlear implants.
